ACL Graft Selection
Once the ACL is ruptured, surgical treatment requires reconstructing, not repairing, the ligament. Previous studies have shown that attempts to repair the torn ligament by sewing it back together were unsuccessful. Therefore, current surgical techniques involve taking a tissue from somewhere else and creating a new ACL; this is called reconstructing the ACL.
This tissue, called a graft, can be taken from somewhere else in your own body, in which case it is termed an autograft, or it can be taken from a cadaveric donor, in which case it is termed an allograft. Frequent sources of autograft tissue include the middle-third of the patellar ligament and the hamstring tendons.
There are pros and cons of both autograft and allograft tissue.
The ADVANTAGES of ALLOGRAFT tissue include the following:
1) Surgical incisions are smaller because no tissue is harvested from your knee. This leads to improved cosmetic appearance.
2) Typically less pain is experienced in the first 3 months following surgery because no tissue is harvested from your knee.
3) There is a decreased risk of developing stiffness after surgery.
4) The risks associated with harvesting the graft from your knee (see below) are avoided.
5) Because no tissue is harvested from your knee, surgical times are typically shorter when allograft tissue is used.
The DISADVANTAGES of ALLOGRAFT tissue include the following:
1) Because the graft is coming from another person, there is a theoretical risk that your body could reject this graft. Although this risk is theoretical, this has never been reported to occur in the setting of ACL reconstruction.
2) Because the graft is coming from another person, there is a theoretical risk of a disease, such as a virus, being transmitted from the graft to your body. Examples of viruses that may be transmitted include HIV and hepatitis. The estimated risk of viral transmission is approximately 1 in 1.6 million but no cases of viral transmission have been reported since 1991 when tissue banks have improved their screening processes for potential donors and updated their “sterilization” processes of the grafts.
3) Animal studies suggest that allograft tissue takes longer to “incorporate” in your knee and become a new ACL. This may have implications for patients attempting to return to competitive sports in a timely fashion.
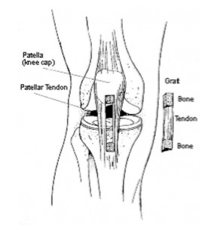
Patellar Ligament Graft
4) Some studies have suggested that there may be a tendency for increased laxity in the long-term when allograft tissue is used for ACL reconstruction.
The ADVANTAGES of AUTOGRAFT tissue include the following:
1) Because the graft is coming from your body, there is no risk of graft rejection or viral disease transmission.
2) Animal studies suggest that autograft tissue “incorporates” into your knee quicker. This may have implications for patients attempting to return to competitive sports in a timely fashion.
The DISADVANTAGES of AUTOGRAFT tissue include the following:
1) Because the graft must first be harvested from your knee before it can be reimplanted into the location of the new ACL, larger surgical incisions are required and longer operative times are needed when autograft tissue is used.
2) Because the graft must first be harvested before it can be reimplanted, patients typically have greater amounts of pain for the first 3 months following surgery when compared to patients who undergo ACL reconstruction with allograft tissue.
3) There are potential complications or consequences associated to harvesting the graft from your knee.
a) When the patellar ligament is harvested as the autograft, there is a risk of fracture of the patella, disruption of the patellar tendon after surgery, injury to one of the nerves under the skin in the area of the incision that may cause numbness on the outside aspect of the leg, or pain in the front of the knee that is worse with kneeling and squatting activities.
b) When the hamstring tendons are harvested as the autograft, there is a risk of weakness of hamstring muscle function, especially with deep knee flexion activities.
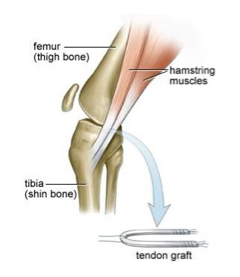
Hamstring Tendon Graft
Overall there are few, if any, long term differences between ACL reconstruction performed either with autograft or allograft tissue.
Most studies suggest no significant long-term differences between allografts and autografts with regard to pain, giving way in the knee, measurements of laxity in the knee, rate of graft re-rupture, rate of return to sporting activity, and overall functional results.