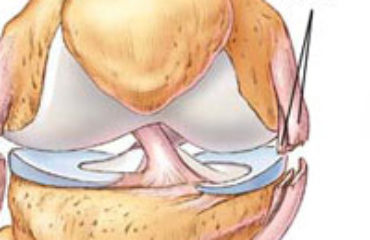
The knee is a hinge joint made up of three main bones: the femur (thighbone), tibia (shinbone) and the patella (kneecap). Holding the knee together are four (4) bands of connective tissue known as ligaments that provide stability against forward, backward, and lateral movement of the knee. The ligaments that hold the knee together are the: the medial collateral (MCL), lateral collateral (LCL), anterior cruciate (ACL) and posterior cruciate (PCL) ligaments. The ACL runs diagonally in the middle of the knee, preventing the tibia from sliding out in front of the femur, as well as providing rotational stability to the knee.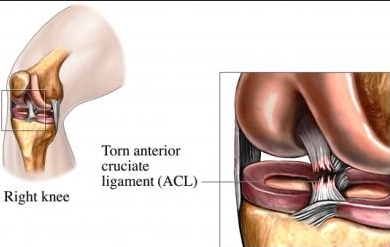
The ACL is one of the most commonly injured ligaments of the knee. There are over 200,000 annual ACL injuries in the United States alone. ACL injuries are more common in athletes that play sports involving a lot of stress to the knee joint, particularly from sudden movement or impact. These sports include, but are not limited to, basketball, skiing, soccer, and football. While direct trauma to the knee can cause injury to the ACl, around 70% of ACL injuries are via non-contact mechanisms.
The extent of ACL injury can vary from strain (Grade I sprains), to partial tears (Grade II sprains), to complete tears (Grade III sprains). The treatment of ACL will vary depending on the severity of the injury, and the individual circumstances of the athlete. Discussion with an orthopedic specialist is recommended prior to any decisions to be made.
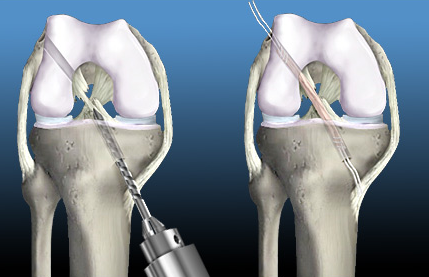 ACL reconstruction is a misnomer, since a torn ACL cannot be sewn back together. The procedure is the surgical graft replacement of the torn ligament with a tendon that is harvested either from the patient’s own body, or from a cadaver. Grafts that are taken from the patient are called autografts, while grafts from cadavers are known as allografts. Allografts are associated with a higher risk of graft rejection, and may require repeat surgery. The most commonly used grafts are autografts using the patellar tendon, or one of the hamstring tendons.
ACL reconstruction is a misnomer, since a torn ACL cannot be sewn back together. The procedure is the surgical graft replacement of the torn ligament with a tendon that is harvested either from the patient’s own body, or from a cadaver. Grafts that are taken from the patient are called autografts, while grafts from cadavers are known as allografts. Allografts are associated with a higher risk of graft rejection, and may require repeat surgery. The most commonly used grafts are autografts using the patellar tendon, or one of the hamstring tendons.
The main advantage of ACL reconstruction is that it provides definitive treatment for the tears, particularly for complete tears of the ACL. Patellar tendon autografts, in particular, are considered the gold standard for ACL reconstruction. Continuous advancements and innovations in surgery have also pioneered surgical techniques that are less invasive, and lead to less intraoperative damage to the knee. Recovery from the surgery can take up to a year, and a recovery program of physical therapy and rehabilitation is important to return to normal function.
The disadvantages of ACL reconstruction include the risk of persistent postoperative pain, and the presence of postoperative stiffness, despite the surgery. There is also the risk of graft rejection from allografts, and graft failure can occur even with autografts. Aside from these, there are the general risks of surgery, such as infection, intraoperative damage to the surrounding muscles and tissues, as well as bleeding and hematoma formation. However, these risks are typically manageable and ACL reconstruction is known to be a well-tolerated procedure with acceptable complication rates.